

The truth about masking
Returning to a scientific civilization


In 2016, the FDA banned the antimicrobial triclosan in hand soaps, in part because of the lack of evidence that it worked better than plain soap and water at preventing infection.
You might wonder how an antimicrobial could not “work”. The issue lies in what it means to work. Here it meant to prevent infection in humans, beyond the baseline effect of soap and water, which already removes quite a bit of pathogen from the hands. “Killing germs” doesn’t necessarily translate into reduced infection — it’s an empirical question, answered by rigorous scientific research.
There’s been persistent disagreement in the US over whether masks reduce COVID rates in the real world. A key error in media and academic discourse is to assume that masks work because they catch some percentage of droplets in lab studies. The percentage is arbitrary, as are the droplet sizes — there’s no a priori knowledge that if masks catch X% of droplets of size Y in a lab, then they’ll reduce infection by K% in the real world (for any pathogen or SARS-CoV-2 specifically). Masking proponents are happy to report — and seem impressed by — any arbitrary numbers for X or Y.
This error suggests a profound lack of insight into the complexity of the behavioral and physical system here — humans walking around breathing through fabric face coverings and the infection processes for this particular pathogen. It’s dumbfounding to see scientists talk as though we can know something like real world mask efficacy without doing rigorous scientific research on the actual variables. Life is full of surprises, and science is even fuller. Any scientist should intuitively understand how surprising reality can be, and how it takes rigorous, valid research to get a handle on it.
If masks don’t work, mask propaganda might well have gotten people killed (even just if cloth masks don’t work). I’ve seen no discussion of this possibility in legacy media. I don’t expect a credible death toll to be huge in this case, but it’s important to understand that there are mortal risks in getting the reality of masking wrong from either direction.
In this report, I want to stress the following:
Some quick steps to cleanly approach scientific questions and cut through political propaganda
Three errors common errors on this other scientific topics: Wrong Variable, One Variable, and Negative Zero
The need to read
Before proceeding, let’s clarify what we’re talking about. SARS-CoV-2 is a respiratory virus with a highly variable risk profile. It has an infection fatality risk of less than 0.1% overall. It poses no mortality risk to most people, but it’s difficult to get details. It looks like it doesn’t kill young, healthy people, where “young” might be under 50, or even older. For minors, the IFR estimate in the linked study is 0.0015%, which is on the high side compared to other sources.
Wrong Variable Fallacy
The outcome variable of interest is COVID infection rates or risk. It is not filtration performance for droplets of a given size. Don’t trust an “expert” who doesn’t understand the difference. There are many miles of ocean between: 1) filtering X% of droplets of size Y, and 2) reducing real-world COVID infection rates.
A basic background fact in biomedical science is that nothing has to work. We can’t make assumptions about extremely complex, invisible physical processes. It’s been disturbing to see purported scientists just assert that masks work, or that cloth masks are better than nothing. They may not be. To illustrate, imagine wearing a fishing net over your head. Is that better than nothing at reducing COVID infection risk in either direction? Presumably not. Keep going. How about a thin, ironic t-shirt, one you can partly see through? Better than nothing? Now go a bit thicker, a bit less ironic, like a Hanes Beefy-T, and you’re approximating a typical cloth mask. What changed that makes you think this semi-permeable barrier “works”? How do you imagine that it works?
A key background fact to understand masking science is this:
An arbitrary reduction in pathogen population (pick a percentage) doesn’t necessarily reduce infection risk.
This is especially true given an arbitrary baseline.
This is true on your hands, kitchen counters, and in the air you breathe. Returning to the FDA example, yes, triclosan kills germs. Yes, we can see it doing so in labs, and it surely kills germs in the real world. Yes, “it’s just physics”. It doesn’t matter. Killing germs isn’t the variable of interest. Infection is.
More concretely, if the pathogen level in a store is X (assume some unit of virus per volume of air), and masks filter 40% of certain droplet sizes, and this leads to a 12% reduction in COVID pathogen being exhaled and inhaled, on top of whatever the baseline environment looks like, this may or may not reduce COVID infection rates in that store. It’s an empirical question. There’s no way to know if masks help without doing rigorous trials. The bottom line is that catching X% of droplets of size Y just might not matter.
Possibilities
Some people have trouble imagining how masks couldn’t work, so I’ll take a moment on this before moving on. The structure of their intuition is unclear — no one has researched it. There are many potential reasons why masks might not reduce infection in the real world, even if universally and properly worn. We’re talking about a very complex system encompassing human behavior, movement, airflow, infection mechanisms, etc. When you change one variable in a complex system, you typically change other variables. When you strap masks on humans, that’s not the only variable you’ve changed. Any decent scientist or epidemiologist should be able to quickly think of a few reasons why properly and universally worn masks of a given type might not work. Here are a few:
The reduction in pathogen population just doesn’t matter in modal settings. Maybe it’s not enough. (This is easy to imagine for schools where kids sit in the same room for six hours — it would be remarkable if a piece of cloth reduced infection rates in that context.)
Changes in breathing behavior/patterns result in less of a pathogen reduction than expected. For example, if people breathe more forcefully, at a faster rate, a less optimal direction, or through the mouth more, wetting the mask (esp those who have constricted nasal passages to begin with, due to allergies, adenoids, etc). There are lots of angles and details here to sort out if it turned out that masks didn’t work.
Masks collect pathogen, leading to repeated opportunities to inhale the same pathogen, or increase touch-mediated infection (hand to mask, then hand to nose or mouth, then eventual inhalation/migration). As above, this gets complicated quickly.
Changes in behavior driven by belief in protection. This is a different level of analysis, could offset a reality that masks do work at the focal level. Behaviors like more time spent in infectious settings, or doing things you wouldn’t do if you didn’t believe masks significantly reduced your risk of infection or infecting others. (This is why propaganda that masks work (even cloth according to Google/YouTube) might have killed people.)
Masks filter other things that help prevent infection. I see this as a reach, not knowing anything at all about this science, but I wouldn’t be surprised if we learned that masking creates a more favorable environment for infection in the airways, a cleaner environment so to speak. Think dust, pollen, the microbiome, effects on mucus composition, etc. If so, masks could offset a reduction in pathogen population by increasing the potency of the remaining pathogen. Or some other mechanism.
The Black Mirror Effect. Another reach. This is my name for the psychological and emotional effects of a masked society, which I expect are negative for most humans, including non-conscious effects. Perhaps depressive and other effects weaken people with respect to COVID infection, the course of such infections, severity, etc. (Only the infection part applies to the mask efficacy question.) The effects of depression, despair, anxiety, hopelessness, etc. on the body, immunity, and disease are not well understood (and might be overstated) — this is just an idea to throw out there, but it wouldn’t surprise me if panned out.
Every single one of these ideas could be false. I have no idea. This is just moment’s-reflection hypothesis generation that any scientist should be able to do on demand. Masks might actually work, in one or both directions. Even surgical masks. As crazy as it sounds, cloth masks might work. Life is full of surprises, and science is even fuller.
But if it turns out that masks don’t work in realistic conditions, we’d want to do the research to unpack why. Some of the above ideas might pan out, or not.
RCTs vs everything else
The way to research mask efficacy is through randomized controlled trials (RCTs). RCTs set in the real world do two things:
They lock onto our variables of interest.
Intervention: Humans wearing masks in the real world
Outcome: COVID infection among those humans, either assessed as a whole or narrowed down to focal risk in places like nursing homes, schools, or even for individuals
They control for all factors except masks, isolating that specific intervention.
RCTs give us our variables, and they isolate those variables. No other research method does this.
Lab studies of filtration performance by droplet size are missing both our intervention — humans wearing masks in the real world — and our outcome variable of infection.
Observational studies might look at our outcome variable of interest, but they don’t isolate the intervention or even measure it. For example, they might compare states with and without mask mandates, but that’s not our variable. We want mask use, and many people wore masks in areas where it wasn’t mandated.
Moreover, such studies don’t control for all other factors, which become extremely messy when comparing entire states. They also depend on third parties to collect and report outcome data instead of handling it themselves, typically government agencies spanning many jurisdictions, so I wouldn’t be confident in the accuracy and commensurability of such data. Finally, researchers haven’t accounted for the conflict of interest of states that passed mandates being motivated to report good effects, or the inaccurate data coming from government agencies. (For example, the CDC overstated child COVID deaths by at least 24%, and its consistently sloppy work has been repeatedly corrected by an alert citizen scientist in Georgia.)
Observational and new methods might be useful, but to know how useful and valid they are, we have to validate them with RCTs. This is often overlooked — RCTs give us our cleanest read on reality, so if other methods don’t agree with RCTs, it would help us improve those methods, find variables we missed, etc.
Note: I see lots of assertions that masks work but only for source control, or when properly worn, or universally worn, or that “quality” masks “work”. There is no RCT evidence for any of these claims. There is no RCT out there that found that masks work if 90% of people wear them, or if 90% of those wearers wear them properly, or any other percentages. There is not a single RCT finding a significant reduction in COVID spread from masking. Not one.
How to navigate scientific questions
Let’s step back. For any scientific question, I recommend the following steps:
What’s the question? Nail it down. Be sure to clarify the variables.
How can we answer this question? What sort of evidence do we need, how much of it, etc.?
What evidence do we have? Go look and find out. It’s critical to to work through the first two steps first — it’s easy to be misled if you start with Step 3.
Does the necessary evidence exist? Is there enough, and does it cover all the key ground? If no, then we don’t know the answer to the question.
Let’s do it now.
The question: Do masks (each type separately) reduce COVID infection rates/risk in the real world, specifically in American/Western settings?
How do we answer it? We need randomized controlled trials for each mask type. Mask trials are about as easy as science gets, and cheap — much easier than developing new vaccines or battery chemistries. There are lots of ways we can achieve high compliance to assigned conditions, and we could set up test towns as well. With modern tech like smartphones and location tracking, we could go gangbusters in checking for confounders and answering subsidiary questions.
What do we have? No trials have been conducted except DANMASK, which isn’t good enough to use, and found no significant effect anyway (surgical masks). The Bangladesh study wasn’t a randomized trial with individual assignment, the paper is littered with data errors, it mostly assessed outdoor masking, most participants didn’t wear masks, its researchers weren’t blind to condition (and administered both conditions(!)), found no significant effect of cloth masks, no effect of surgical except for the elderly, its reported effects are based on 20 cases in over 300,000 people, the researchers were politically biased, and it was in Bangladesh. More in Appendix A.
Do we have the evidence we need to answer the question? No, the one trial found no effect, and the Bangladesh mishap has no epistemic standing, should never have been published, and had mostly null findings anyway. We can’t claim masks work, nor can we claim that they don’t. Any type, any direction. We’ve got nothing. (I disagree with people who say masks don’t work. We don’t know if they work, because we haven’t done the work to find out.)
A common mistake I see in leftist culture is to assume that whatever “science” happens to exist on a topic right now — today — can definitively answer whatever question we’re asking. (I use “leftist” simply as left-of-center, Democratic voters, etc. I have little use for left-right framing, since there’s no symmetric opposite of leftist ideology and the intellectual landscape is multidimensional, but I’m stuck with the labels. I won’t use Orwellian, question-begging terms like “progressive” — I’d prefer something like massco, since leftists favor mass coercion across domains.)
First, it’s important to understand that this is an arbitrary place and time for humanity — we just happen to be alive right now. Science is young, and in academia it’s low quality, unreliable, and subject to profound political biases. Science isn’t a vending machine that spits out answers to whatever we’re asking, and many questions are not answerable given our current scientific abilities.
Second, it’s easy to be fooled if you just go hunting for “studies” without thinking through what sort of evidence we need. In a case like masking, if you don’t know why we need RCTs you could easily be fooled by observational studies, especially if you don’t read them.
Sometimes the evidence we need simply doesn’t exist, and that’s before we get to issues of reliability, bias, and fraud. That’s the situation for most questions. We just don’t know. If we don’t do the research – the right research – we won’t know. I see so many writers at leftist media outlets just assume that whatever appears in search results when they roll out of bed on any random day is sufficient to answer the question. This, combined with their Wrong Variable Fallacy and ignorance of the need for randomized trials, led to lots of misinformation.
Negative Zero Fallacy (NZF)
I call this the Negative Zero Fallacy:
Question: Do masks reduce COVID spread in the real world?
A study comes out reporting no significant effect. (It doesn’t matter what kind of study.)
This study is debunked. (Let’s just grant this for our purposes.)
See, masks do work! It’s false to suggest that they don’t.
Wrong. A null finding doesn’t become evidence in favor of efficacy by being debunked. We’re still left with no evidence of efficacy. We’re just negating zero at that point. (I borrow the negative zero concept from computing, where floating point decimal number systems include negative zero.)
In addition to 1) citing an animation of a mask as evidence, and 2) quoting a random MD in Minnesota who just asserted that masks work (he was chosen because he’s a maniacal leftist on Twitter), Politifact claimed that 3) the DANMASK trial had been debunked. The result of 1, 2, and 3 is zero evidence of mask efficacy. It didn’t occur to them that you need evidence for a claim to justify the claim — the burden is always on those making a claim. Politifact is a leftist censorship group that targets non-leftist discourse and gets it censored by Facebook, including facts and even opinions on matters of opinion. Here they tried to justify YouTube’s censorship of Sen. Rand Paul’s claim that cloth masks don’t work.
Likewise, leftists immediately scrambled for ways to dismiss the Cochrane systematic review of randomized trials of mask efficacy for respiratory viruses, which found no evidence of benefit. Debunking such a conclusion (which they didn’t do) still leaves us with no evidence of benefit, since Cochrane didn’t exclude any trials. If anything, Cochrane was too generous in my view in including the Bangladesh mishap, a study that wouldn’t normally meet the inclusion criteria for a meta-analysis. The lack of COVID-specific trials might have led them to loosen their standards. (When I first heard that Cochrane had done a review, I was confused. A review of what? There’s hardly any research to review, so I wondered if I’d missed some.)
The VR forest
We currently face a structural epistemic problem that makes truthseeking more difficult: Leftists consistently act to censor science that undermines their ideology and narratives (just as they strive to ban or alter books in the world at large). Censorship combined with the left’s authoritarian epistemology makes it easier to point to “experts” to bolster leftist narratives.
It’s difficult to get academic journals to publish anything that contests leftist/mass coercion ideology, and academia discriminates against non-leftists and high-integrity leftists, so there are very few academics who would attempt to publish anything contesting mandatory leftist beliefs. One university fired a professor for arguing that there was no evidence to support the campus masking mandate or forcing college students to get COVID shots. (I’m not aware of published favorable risk-benefit analyses for that age group, and the unknown long-term effects of new/experimental pharma would require a significant weight assigned to those risks. Leftist beliefs that the shots prevent transmission were false.) Apparently, that’s the entire story — there was no other basis. The same university (Southern Maine) put a professor through Maoist “restorative justice” sessions for simply noting that there are two human sexes, and Harvard drove out a lecturer for noting that same basic fact. Such cultish denial of basic facts, and demonization and otherization of those who state them, strips the core commitment to truth that science requires.
When research contesting leftist narratives does get into journals, leftists will swarm to call for its retraction. See Appendix B for six journal articles retracted by leftists for political reasons in just the last three years, including articles on the purported harms of masking (there will be more — I just happened to know of the six offhand, from bits of non-leftist media coverage and X/Twitter). That leftists would fiercely advocate humans masking was unexpected, seemingly arbitrary with respect to their ideology, but they often adopt arbitrary empirical beliefs, which they then politicize, stigmatizing and censoring dissent. We saw this with their campaign to keep schools closed, false claims about natural immunity, a seemingly permanent and extremely dangerous bias against any claims or discoveries of negative effects of the still-experimental COVID shots or even against rigorous risk-benefit analyses, and the once plausible and now likely lab origin of the COVID virus (Ashley Rindsberg capably documents the latter story here). Leftists often take arbitrary positions based on what they think conservatives/Republicans believe (such beliefs might be news to most conservatives). For example, Levison, Geller, and Allen (2021) report that leftist teachers lobbies were set to call for American schools to reopen in Fall 2020, but instantly reversed their stance when President Trump called for the same.
Leftist bias and censorship makes our task more difficult. Whatever studies we see are those that survived academia’s political bias, adding another layer of publication bias. Moreover, it’s wise to assume that those that advance leftist narratives are held to low standards, like the Bangladesh study. This is a systemic problem that needs systemic fixes, but the best thing you can do for now is to read any studies, carefully. That alone will pay big dividends. I also recommend getting the data and examining it. If the data isn’t available, and the authors refuse to provide it, I’d toss the study (journalists should definitely do this). In general, I’d be skeptical of any academic claims that support leftist narratives. I’m confident in predicting that the majority of such claims are false or invalid (making the claims unsupported, and likely false) — we need a systematic assessment of academic research and claims so that we can provide deeper insights here and concrete numbers.
The One Variable Fallacy
So far this essay has been an exercise in barbarism. COVID infection is just one variable people care about. It’s just one aspect of biomedical health, and humans have many values beyond biomedical health. Masking has many harms — it impairs verbal communication, facial recognition, and emotion display, and facilitates crime. We should expect it to dehumanize people in various ways. For some of us universal masking is depressing, feels dystopian, while for others it might be inspiring if they think it marks a communitarian commitment to save lives (this assumes masks reduce COVID spread, which we have little reason to believe so far). Masks also impair learning in young children, and if you believed claims that they didn’t, you might retrace your steps and reflect on why you believed such a claim, and whether you’ve accepted other implausible claims because they came from media or government.
Do you know any couples who met randomly in public, say at a store, park, or ballgame? Masking snuffed out a large number of love stories. Those scenarios largely depend on faces, what people see in someone’s face, and the communication interplay that faces afford. Relatively few such scenarios will unfold between masked people (though there must be some). This effect is exacerbated by lockdowns and the cancellation of various events.
Humans have every right to care about more than one thing, e.g. COVID infection risk. They have to right to weigh biomedical harms against the harms noted above, or any others, and to build frameworks to help assess tradeoffs. They might also oppose forced masking on ethical or principled grounds, perhaps viewing such coercion as unjust in the context of this particular pandemic, with its particular characteristics, or in any realistic pandemic. Americans also might not trust “public health” authorities, and at this point they’d be justified given how non-rigorous, unintelligent, and politically craven American authorities were. They certainly have every right to say No to whatever this is:
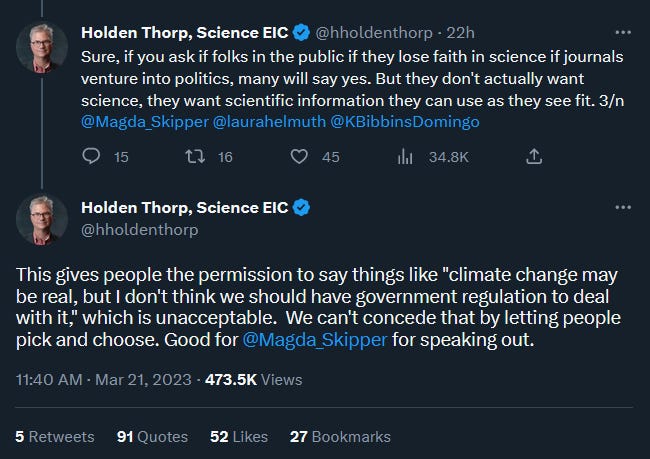
We’ll return to Thorp in Appendix A.
Relatedly, I’ve been talking like a barbarian about whether “masks” “work” as though we can meaningfully talk about it so simply, without any elaboration or quantification. I didn’t want to get bogged down early with all the qualifications and complexity the issue ultimately requires. Instead, I chose to mirror the way the media and simple-minded “experts” commonly talk about masks.
“Masks” needs to be broken down into cloth, surgical, and N95 at minimum. Leftists stridently asserted that they all “worked”, and censored US Senators like Rand Paul for saying that cloth masks don’t.
And “works” needs to be explained and quantified. In which direction? How much do they reduce infection risk or rates? In other words, what’s the effect size? In what conditions?
If universally and properly worn surgical masks would reduce COVID infection rates by 11% in typical American setting, and COVID has an infection fatality rate of less than 0.1%, people might decide masking isn’t worth the harms.
Of course, that assumes that (surgical) masks have such an effect, which has never been established, and my hypothetical requires universal and proper use. Anyone arguing for forced masking needs evidence that forced masking works — we’d need to know that whatever masks people would wear, with realistic estimates of proper use, reduce COVID rates by X percent. With credible estimates from RCTs we could then have a conversation about the benefits and harms, the human rights issues, etc. In the US, we never got that far, never commissioned the RCTs or had any discussion of the harms of masking in light of quality evidence of benefits.
Moreover, it’s not clear how we should account for the inevitability of COVID infection. If masks have some effect, does that imply a delay in getting COVID for some people? Are we talking about a slight reduction in the average number of times people got COVID by, say, the end of 2021? Masking could never be permanent, so it’s unclear how they’d ultimately help since COVID will be with us for thousands of years. (I have no idea if getting COVID in 2020 vs 2021, or in general earlier rather than later, is better or worse — I assume it’s not a wash.)
The pandemic was a blur for me, but I’ve since learned what happened in retirement homes, how families were kept from seeing dying elders, and how residents and staff were masked during elders’ final chapter on this earth. I don’t like thinking about how inhuman we made their lives. It’s another context where we need to bring in that there’s more to life than staying alive (and the premise that masks work in such persistent 24/7 settings may well be false).
Ethics
When the lack of quality scientific evidence for mask efficacy is exposed, leftists often retreat to assertions that it would be “unethical” to conduct masking trials. The idea is that the participants randomly assigned to the no-mask conditions would be at greater risk of harm from COVID infection, and that for some reason we can’t allow adults to consent to such a risk.
This argument rests on a severe error — the assumption that masks work, which is the very question we’re trying to answer. It’s the fallacy of begging the question. That American academics and media people are operating at this level of intellect is a bad sign for the state of our civilization.
A deeper issue is that leftists often conflate ethics with their political ideology, and say “That’s unethical” as though it’s a descriptive fact, like saying “Today is Tuesday”, often citing a written artifact. This can be confusing, as it implies that they don’t understand the difference between descriptive reality and normative ethical views, that their opinions on ethics aren’t universal, the layered ideological assumptions and non-universal value judgments underneath their assertions, and the range of other perspectives. As sage philosopher Oscar Martinez succinctly noted, “Ethics is a real discussion of competing conceptions of the good.” I’m confident that most humans around the world — and most Americans — would disagree with the claim that it’s unethical to allow adults to consent to participate in masking trials.
Needless suffering
It troubles me that leftist leaders, academics, media people, etc. haven’t clearly told their followers that masking outdoors is completely pointless. Many leftists are confused, and are living in fear that they simply don’t need to be living in. In the San Francisco Bay Area, I’ve seen people on leisurely walks in residential suburban neighborhoods and even cyclists wearing masks. Leftist outlets included “Best mask for running” in their eager mask reviews. Whatever we think we might find if we do the trials on indoor masking, academics and public health officials should be honest and crystal clear that masking outdoors is ridiculous. They should use strong, unequivocal terms. There’s no reason to continue to let leftists live under this delusional belief that masking outdoors is doing something.
There might be an issue with leftists’ understanding of outdoor airflow dynamics specifically, even though it makes no sense for a political ideology to sprout such an issue. I say this because leftists not only fear incidental exposure to second-hand tobacco smoke, but fear outdoor exposure to it, and have banned outdoor smoking in many settings. The case for the harms secondhand smoke is weaker than initially believed (never believe the first round of “scientific consensus” on politicized issues), and that’s entirely about chronic indoor exposure — forget about fleeting outdoor exposure. Leftists consistently seem unaware of dose-response, even an intuitive lay understanding. We see the same dynamic with their growing fear of “indoor air pollution” in their homes. A good example is Sam Harris’ The Fireplace Delusion essay (2012) arguing that occasional use of a fireplace is harmful to a normal human’s health. The essay is a stunning collapse of scientific rigor, logical reasoning, and awareness of dose-response that seems rooted in a neuroticism so severe that it should be professionally treated (and it foreshadows Harris’ maniacal COVID fears and similar lack of scientific rigor, or even engagement with science).
Fear of invisible inhalants is recurring theme in leftist culture, and it might represent an important psychological trait or cognitive framing. It’s definitely worth researching — if only we had institutions that formally, rigorously researched human psychology, including political psychology and cultures…
Leftists don’t trust outsiders. They’re trained not to. At this point, anything that diverges from their belief system — even newly acquired, arbitrary empirical beliefs — is likely to be coded as “right-wing”, “far right”, or even linked to Donald Trump. Built into leftist ideology is a formal focus on the “motives” of outsiders/dissenters, and a methodology that skips to who is saying something rather than the substance of their claim and its epistemic status. They even look to who else is saying something (or what else a masking skeptic says on other topics), such that if Vladimir Putin was skeptical of mask efficacy, this would actually matter to leftists, and lead them to link masking skeptics to Putin. This is one reason why leftists are unable to successfully navigate scientific topics. Not only do they lack any training or framework for it, as well as a formal commitment to truth and integrity in their ideology, but they’re trained to focus on politics, tribal in-group dynamics, reinforcing their prejudices toward the “right”, etc.
All this means that the truth has to come from their leaders, media, etc. They simply won’t believe outsiders, conservatives, libertarians, apolitical scientists, dissident leftists, etc. It’s long past time for leftist academics, TV anchors, and “experts” to tell their followers the truth. There’s no reason to let people live in fear of going outside, or to suffer and pepetrate the harms of masked faces for a hypersocial, face-salient species.
Humans must read
This world would be dramatically better overnight if people would just read. It often feels like no one is reading anything fully or carefully. The American CDC put up an anonymously written masking science page full of false statements, including false descriptions of study conditions, false descriptions of results, and false sources. The page is junk. They also excluded something very obvious from their table, and included the story of the two hairdressers. Apparently no one noticed. I saw three false statements in just my first reading. It helped that I’d read some of the studies they mentioned — without that, I wouldn’t have caught two of the errors.
A nation of 330 million people, a $21 trillion GDP, and over a dozen major media outlets needs to be able to get eyes on CDC “science briefs” and notice the false claims. Our culture is failing to deploy a baseline of active, attentive intelligence, and that’s dangerous.
Similarly, academics and science writers should’ve noticed that all of sudden leftists were citing differences in masking studies without disclosing that they weren’t statistically significant (see Appendix C). I’ve never seen this before on any topic. Leftists abandoned, in seeming unison, a basic standard of scientific rigor and guardrail against spurious claims. Note that whatever one thinks about the emphasis on p-values or the right threshold for p-values, we cannot simply report differences without disclosing whether they were significant by the framework the researchers used. There’s no denying that this practice is corrupt when these partisans only do this for masking studies that don’t go their way, while stressing the lack of statistical significance for, say, ivermectin studies — another arbitrary empirical issue on which leftists took a dogmatic position at Time 1. (Most ivermectin studies show the ivermectin group faring better, but the difference is usually not statistically significant, though chunky in human terms, e.g. a day of recovery. Complete list here.)
Regarding observational studies, I repeat my message. Read them. I’m setting up a bit of a trap here. I know what’s out there. You should be able to toss some of the observational studies before you get to the results, if you just read carefully, but I’m confident no one will pass this test. I don’t think anyone will notice obvious validity errors, but I hope to be pleasantly surprised. In any case, no one should cite studies they haven’t read carefully. Academia has the lowest standards in our civilization, in terms of rigor, integrity, and increasingly, intelligence — much lower standards than private sector financial reporting, for example. We can’t do anything with academic research without carefully reading it and examining the data. It’s long past time that we systematically address this issue. A talented team with a tailored version of ChatGPT or Grok could identify a large number of false and/or invalid peer-reviewed journal articles (likely most articles in some fields, like social psychology, my field), rate the epistemic risk of all articles, separately identify all research for which the data doesn’t exist (most), etc. If this interests you, contact me.
Joe Duarte earned his doctorate in Social Psycholgy at Arizona State University, where he was a National Science Foundation Graduate Research Fellow. His interests focus on scientific validity, political bias and falsity in the fact checking/censorship sector, and how political bias in academia undermines research claims. You can reach him at gravity@protonmail.com.
Appendix A: The Bangladesh masking study
Reading through this study just once exposes this fractal hell:
Not a randomized trial at the individual level, just villages in different mask propaganda and distribution conditions.
Most people in the masking arm didn’t wear masks. (But we can’t believe the numbers anyway.)
This is mostly a study of outdoor masking, plus inside mosques. We should be extremely skeptical of effects of outdoor masking, given everything else we know, the NCAA football study, etc. An outdoor masking study where most people didn’t mask anyway isn’t worth talking about.
The same researcher-observers rated both masking and control villages. They weren’t blind to condition, and the study handed out unique, custom designed masks…
The difference between the two groups is 20 cases of seroprevalence. Twenty. We can’t possibly trust research based on 20 cases in such an enormous sample, and we can’t be confident in the accuracy of a six-figure sample size. All the math depends on the sample size and groups sizes being perfectly accurate…
The authors never disclose the number of cases, but Ben Recht has them here. I’ll stop there. We’ve simply got to get more people to read, and think.
It’s worth talking about the journal that published this junk, and the alarming bias of the lead author.
The journal
Someone will have to contact Science about the errors — they won’t care about the catastrophic invalidity of the research (points 1-3) — but I’m not confident in this journal. Editor Holden Thorp is an unhinged, hyperpartisan maniac, not a man of science. For him, science is a tool of mass coercion aligned with his political ideology:
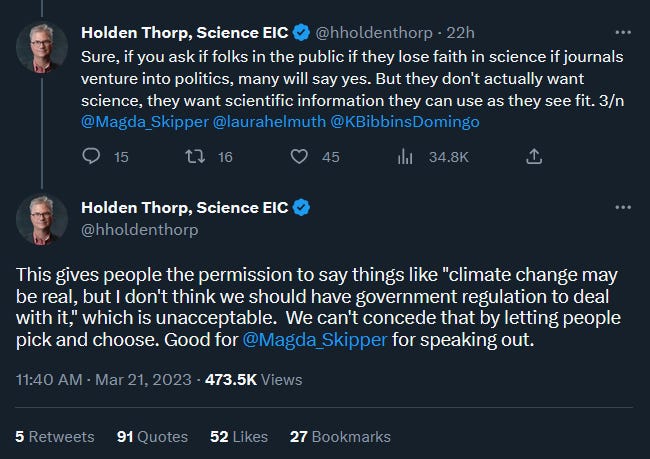
Beyond his sneering totalitarianism, note his lack of intellectual rigor — that x is “real” is assumed to justify government coercion (and it will have to be his tribe’s preferred policies). Dissent is “unacceptable”. That x is something as vague, complex, inevitable, and arguably irrelevant as “climate change” only makes it worse. There’s no trace of a coherent epistemic, ethical, or human rights framework in this ideology of “x is real, therefore do something!” (and it ignores issues of equal or greater realness, like crime, the collapse of education in “blue” cities, unprecedented illegal immigration, the mutilation, sterilization and drugging of tens of thousands of children on leftist “trans” grounds, federal spending, censorship, the mental health impact of delusional beliefs about climate change being an existential threat, the misinformation about the experimental COVID shots spread by authorities and academics, pervasive fraud and falsity in academic output…) Leftist academics are just lay leftists — they have the same false beliefs as any MSNBC viewer. They don’t do anything to check their beliefs, read non-leftist media, or have any tools or principles that would mitigate leftist bias. Being an academic confers no advantages of rigor, education, or tools, and likely has the opposite effect for various reasons.
Thorp was Chancellor at UNC when my program chair there was exposed as a fraud (Lawrence Sanna, chair of the social psychology program, had just taken a job at Michigan). UNC covered it up, pressured the graduate students to sign what sounded like NDAs (I’d transferred out by then), and treated it as an HR issue — unprecedented for scientific fraud.
More recently, Thorp invited me to burn in hell. In a deleted tweet, he invited all NRA supporters to do so (I joined in 2022). He lives in a nation of 330 million people, yet he’ll respond to a random shooting anywhere in the country, depending on the race of the shooter, with unhinged vitriol against non-murderous gun owners (≈99.98%) and the NRA for some reason. He doesn’t seem to care about the murder rate, or the explosion in murders (by several thousand) sparked by his false and destructive BLM ideology in 2020, just a narrow, extremely rare type of media-boosted murder-by-gun. He puts his political ravings in the journal itself, and even publishes fraudulent research that advances his ideology. Science didn’t even respond initially when I notified them that the opening sentence in this article is wildly false, and of another false claim further in, and it’s still uncorrected, unretracted. (Gun violence is not a leading cause of death in the US — not even close. And suicides and accidents aren’t violence, but it wouldn’t matter if you included them that year anyway. It’s just a false claim.)
Clearly, this man should not be the editor of a scientific journal, especially when he uses it to advance his awful totalitarian ideology and his hatred for millions of good people over some sort of political or cultural prejudice. He has no evident commitment to truth as such, doesn’t retract false papers if they advance his ideology, and lacks the intellect to understand complex scientific topics and the difference between descriptive reality and political policy preferences (and the philosophical frameworks they rest on). “Science” for him is an unusually status-conscious occupational guild and a tool for his destructive ideology of mass coercion, not an open-minded, rigorous truth-seeking enterprise.
The author
Finally, the lead author of the Bangladesh mishap, Jason Abaluck, said:
“I think this should basically end any scientific debate about whether masks can be effective in combating covid at the population level.”
This is a stunning collapse of scientific culture. No scientist would ever talk that way after having conducted a single study, even a high quality, well-executed RCT on a much more constrained reality, like the effects of a new antiobiotic. Spend a few seconds pondering points 1 through 6 above, letting the reality of this mishap sink in, and consider his statement again.
When I read that, I immediately knew something was very wrong here, not even having read the study. No serious researcher talks like that. Not ever. You’d have to be a moron to think you settled any debate doing what he did, in Bangladesh of all places, and getting the results he purportedly got. It turns out he’s an economics professor at Yale, a haven for far-left crackpots. It’s not clear why an economics professor is leading an epidemiological study, but he isn’t qualified for such work or any role in science. He simply doesn’t understand what science is, or how knowledge works. There are many layers of error and ignorance in saying what he said about this particular scientific question, multiplied by the nature of his study and results he was referring to. If you ever see researchers talk like this, saying the science is “settled”, “no debate”, etc. — especially after a single study — I’d dismiss their claims. I can’t overstate how shocking his statement is — it’s idiocratic, the opposite of a scientific mind.
Appendix B: Leftist retractions of peer-reviewed journal articles
The following is a quick, incomplete list of nonsubstantive retractions of peer-reviewed journal articles orchestrated by leftists. None of these are alleged fraud cases. We urgently need a complete, systematic accounting of such nonsubstantive retractions, and any trend over time — my impression is that nonsubstantive retractions like these were largely unheard of until 2010 or so. These are just the ones I recalled offhand from reading random media and X/Twitter.
A 2023 review of the physio-metabolic and clinical consequences of wearing face masks. The editors said: "It was found that the complaints were valid and that the article does not meet the standards of editorial and scientific soundness…" of the journal. That’s it — no explanation.
A 2021 experimental study of masking effects on CO2 levels for children specifically. The editors said they solicited a response to criticisms from the authors, but didn’t publish that response or any details of the criticisms.
A 2020 study in Nature that reported worse outcomes for female mentorship of female junior academics vs. opposite-gender pairings. The editors claimed that the results “undermines the role of female mentors and mentees”, as though such an opinion was relevant to a question of fact.
A 2021 pilot study of ivermectin as a treatment for mild COVID symptoms. The journal’s “Founding Editor” swooped in after the fact to unilaterally retract it with a near explicit political rationale: "Additionally, no reference is made to the well-known controversies that surrounded the recommended use of ivermectin to treat infections with COVID-19. The omission of any discussion of these controversies in the present paper makes the paper misleading and unacceptable." It obviously isn’t “misleading” to not discuss a largely American leftist controversy when reporting the results of one’s empirical work. (The researchers are Brazilian.) The editor also made vague methodological claims, but didn’t back them up anywhere.
A 2022 study reporting no upward trend in extreme weather event frequency (an assessment shared by other climate scientists), contesting leftist narratives around a present “climate crisis”. The editors said: "Concerns were raised regarding the selection of the data, the analysis and the resulting conclusions of the article." That’s it — no explanation.
A 2023 survey study exploring the hypothesis that social contagion is a factor in the dramatic increase in American children and young adults complaining of gender dysphoria. The journal first considered a lack of IRB approval as the basis for retraction. Academics normally need IRB approval to conduct a survey, or an expedited stamp of approval that doesn’t go through the full process, but the first author isn’t an academic (no one needs anyone’s approval to conduct a survey in the world at large). They settled on the fact that the survey consent form secured participants’ consent to publication of the results on a website, but not specifically in a journal.
Appendix C: Collapse of standards in reporting non-significant results
I noticed last year that leftists across the media landscape were reporting non-significant results of masking studies without disclosing that they weren’t significant. This is unprecedented in science reporting in my experience, an inexcusable collapse of integrity. You’ll notice that each of these activists finds a different way to dance around it. The word significant never appears. Note that this behavior stands in contrast with how they report ivermectin research results, where they ignore that ivermectin groups fare better and go straight to saying that it “didn’t work” or that the results weren’t statistically significant. (Leftists became obsessed with ivermectin once they perceived it to be something conservatives or Trump believed in — another example of taking arbitrary, dogmatic positions on empirical questions.)
Tom Frieden, former CDC Director, Februrary 23, 2023 on X:
Community-wide masking is associated with 10-80% reductions in infections and deaths, with higher numbers associated with higher levels of mask wearing in high-risk areas.
Cochrane included only two actual studies of masking during the pandemic. The first, from Bangladesh, showed a marked reduction in infections. The second, from Denmark, suggested a 20% reduction but it had methodological problems and limited power to detect differences.
I’m not sure what he’s referring to with the 10-80% reduction claim, and that’s an absurd range to tout. We already know the Bangladesh claim is false — it was only 20 cases in a purported sample of exactly 342,183 people, and the study was invalid anyway.
The Denmark claim is false — it was a 14% reduction, and only 5% when strict maskers were compared to control. In any case, the results were not statistically significant, and he doesn’t disclose this to his readers, dancing around it with “limited power to detect differences”. If someone can reach him to get him to correct, that would be good. He should prominently correct in a separate post, maybe pin it. The problem I foresee is that he’s a leftist, and as we see over and over again, leftists lack a core commitment to truth, integrity, and scientific rigor. Their political ideology and tribal standing are more important to them. We seem to have devolved into a society where people can make flatly false claims and never correct, if they’re leftists.
Nevertheless, they found that mask mandates helped suppress COVID. In one, a massive study of more than 340,000 residents of rural Bangladesh, the study found that mask programs that promoted but didn’t mandate masks “increased mask usage and reduced symptomatic SARS-CoV-2 [that is, COVID] infections, demonstrating that promoting community mask-wearing can improve public health.” Masking trebled among the test group.
The second study, involving about 6,000 Danes, found a modest difference between mask-wearers and non-wearers. But the study was small and underpowered in statistical terms — it was designed to test for a 50% reduction in infection rates, and took place in a setting where COVID infection rates were already very low.
Something else he missed is that the two studies in the meta-analysis that actually measured the effect of mask mandates in the COVID-19 pandemic, from Bangladesh and Denmark, showed that mask mandates did reduce infections and the spread of the virus — quite the opposite of a conclusion that they “did nothing.”
He’s disputing Cochrane by quoting a part of a sentence from the abstract of the Bangladesh study, a study Cochrane carefully assessed. He has no idea what’s going on here, obviously didn’t read the study and doesn’t give his readers any details, e.g. that the study wasn’t blinded, that there was no significant difference for cloth masking, that the only significant effect was for surgical with older adults, that the study centered on outdoor masking, that most people didn’t wear masks in either condition, and of course he didn’t notice that the symptomatic and seropositive percentages in the paper are all false.
With DANMASK, he avoids telling his readers that the results were not statistically significant. He pulls the CDC trick of saying what size difference the study was designed to detect (50%) without disclosing what the observed difference was (≈14%), letting readers think the observed difference might have been just shy of that 50% figure.
He never discloses mask type anywhere here, which is important because leftists have stridently claimed that cloth masks reduce COVID spread, even censoring US Senators like Dr. Rand Paul for saying they don’t. DANMASK used surgical masks. The only significant effect the invalid Bangladesh mishap reported was for surgical masks.
His last paragraph is just false. Neither study measured the effect of mask mandates. There were no mask mandates. In fact, in the first para he explicitly says masks weren’t mandated in the Bangladesh study, yet he says they were in the third paragraph. This man is phenomenal.
Can someone contact the LA Times to get his false claims corrected? The mask mandates claim should be easy for them to understand. Explaining the others might be difficult. They’re a notoriously partisan, unreliable outlet (the left has turned journalism to ash in just a few years), but at some point we need to roll up our sleeves and go to these outlets and pressure them to correct all their false claims.
Zeynep Tufekci, March 10, 2023 in the New York Times:
Of those assigned to wear masks, 1.8 percent became infected, compared to 2.1 percent in the no-mask group — a 14 percent reduction. But researchers could not reach a firm conclusion about whether masks were protective because there were few infections in either group and fewer than half the people assigned masks wore them.
False. The results were not statistically significant. She needs to just say that. She layers false and misleading claims here:
It’s false to say that the researchers “couldn’t reach a firm conclusion” because fewer than half of the mask group wore masks or that there were too few infections. If everyone wore masks and they got the same non-significant results, they wouldn’t be able to reach a firm conclusion for the same reason they couldn’t here — lack of significance. No one knows the reasons for a null finding — you have to actually do rigorous scientific research to find out. Tufekci is a menace, and the more this kind of pseudoscientific hokum is tolerated, the worse off our civilization will be.
It’s also false to say that fewer than half of that group wore masks. 93 percent either wore masks as recommended (46%) or predominantly as recommended (47%). She left out the latter. She also left out that when the comparison was limited to the former vs. the control group, the difference in infection rates got smaller: 2.0% for strict maskers vs. 2.1% for control.
Who wants to contact the New York Times for a correction? It might be hopeless — they reported a 3% mortality rate for COVID as recently as 2023… (it doesn’t matter if it’s IFR or CFR if the claim is 3%). They only employ leftists to write about science, and I don’t think they have any staff who can read a journal article and understand anything beyond a false number that is explicitly provided in the text.
These people are not at all interested in science. "Science" is merely a storehouse of mysteries to be used in magic rituals. They are in fact sorcerors, not scientists. Whenever their words don't make rigorous scientific sense, it is because they are casting a spell and their words are magical devices. Indeed, the simplest, most useful definition of "wokeness" I have found is *activist mysticism,* a term that perfectly captures the propensity for unfalsifiable beliefs as well as the ritual purity used to defend them.